Introduction
If you’ve got pain right at the bottom of your kneecap that gets worse with jumping, squatting, or climbing stairs, there’s a good chance you’re dealing with jumper’s knee, an irritation of the patellar tendon, the thick band of tissue connecting your kneecap to your shin bone.
The good news: it responds well to the right kind of loading; The bad news: “the right kind of loading” is almost never what most people are told to do first.
Here’s the thing — nearly every resource you’ll find on this tells you to rest it. And for the first few days after a genuine flare-up, easing off is reasonable. But if resting is where your plan ends, you’re not actually fixing anything. You’re just pausing it.
Get Your Physiotherapy Treatment Today
Understand your condition better with our detailed physiotherapy assessment, and return to normal life pain-free by addressing your root cause.
Click the button below to book an appointment now!
Treated over 1,000 patients. 30% off first visit
What Is Jumper's Knee
Your patellar tendon is the tough, rope-like tissue that connects your kneecap (patella) to the top of your shin bone (tibia). Every time your quadriceps — the big muscle group on the front of your thigh — contracts to straighten your knee, it pulls through this tendon. Jumping, landing, sprinting, and squatting all send a large amount of force through it in a very short space of time.
Jumper’s knee [a.k.a. patellar tendinitis (short-term tendon inflammation) or patellar tendinopathy (long-term tendon damage)] happens when that tendon is asked to absorb more load, more often, than it can currently tolerate. Over time, this creates tiny areas of damage within the tendon fibres. Left unmanaged, those small areas of damage accumulate.
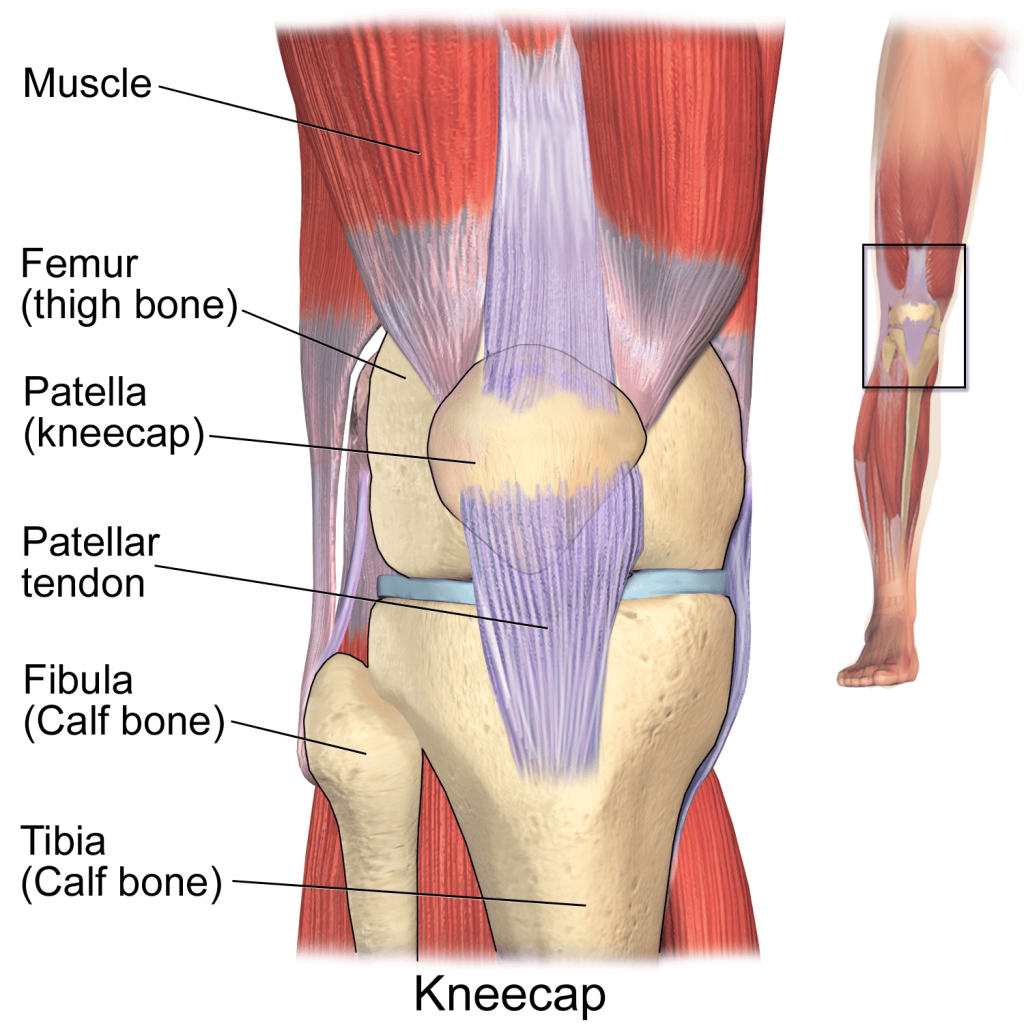
BruceBlaus. When using this image in external sources it can be cited as:Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436., CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
How Do You Know If You Have Jumper's Knee? (Symptoms)
Where the Pain Shows Up
The pain of jumper’s knee is specific and localised — right at the bottom point of your kneecap, where the tendon attaches. Press directly on that spot and, if this is jumper’s knee, it’ll usually be tender. You’ll typically also notice:
- Pain when straightening your leg against resistance, squatting, or jumping
- Stiffness in the knee, especially first thing in the morning or after sitting for a while
- Discomfort going down stairs more than going up (lowering under load is harder on the tendon than lifting)
- A dull ache that can turn sharp during higher-impact movement
Pain That Eases With Warm-Up, Then Returns
This is one of the most useful clues for figuring out what you’re dealing with. Jumper’s knee pain often behaves in a very particular way: it hurts as you start moving, quietens down once your tendon has warmed up and you’re mid-session, and then comes back once you’ve stopped and the tendon has cooled down. Pain during prolonged sitting, kneeling, or at night is also a commonly reported feature.
If your pain follows that on-off-on pattern rather than staying constant throughout activity, that’s a meaningful sign pointing toward the tendon rather than something else going on inside the joint.
When It's More Than Mild — Signs to Get Assessed
Most cases of jumper’s knee are manageable without urgent intervention, but get assessed sooner rather than later if:
- The pain is present even at rest, not just with activity
- You notice swelling around the tendon
- You have sudden, sharp pain and difficulty straightening the knee (this can signal a partial or full tendon tear, and needs prompt attention)
- Symptoms are steadily worsening despite backing off activity
Jumper's Knee vs Runner's Knee: What's the Difference?
These two get confused constantly, partly because they sound so similar and partly because both show up in active people. Here’s how to tell them apart.
Jumper’s Knee (Patellar Tendinopathy) | Runner’s Knee (Patellofemoral Pain Syndrome) | |
Where it hurts | Directly below the kneecap, at the tendon | Around or behind the kneecap |
What’s affected | The patellar tendon | How the kneecap tracks against the thigh bone |
Pain pattern | Eases during warm-up, returns after activity | Tends to worsen the longer you’re active |
Aggravated by | Jumping, landing, squatting | Stairs, prolonged sitting, running downhill |
Typical cause | Repetitive tendon overload | Muscle imbalance affecting kneecap movement |
Can You Have Both at Once?
Yes, they’re not mutually exclusive. Both conditions can trace back to a similar root problem: weak hip abductors, particularly the glute medius (the muscle on the side of your hip responsible for controlling how your leg moves under load). Weak hip abductor strength is consistently associated with both patellofemoral pain syndrome and patellar tendon issues in runners. If your pain doesn’t fit neatly into one box, that’s often exactly why.
What Causes Jumper's Knee? (And Why It's Rarely Just "Overuse")
Repetitive Jumping and Landing Load
The direct mechanical cause is straightforward: repeated high loading of the tendon, faster than it can adapt and recover.
Basketball, volleyball, track and field jumping events, and sports involving a lot of cutting and landing are the classic culprits.
In Malaysia, we see this just as often in weekend badminton and futsal players and in gym-goers who’ve suddenly added box jumps or heavy squats to their program without building up to it.

Muscle Imbalance and the Kinetic Chain
Here’s what most patient education misses entirely: the patellar tendon rarely fails in isolation.
In our experience, the site of pain is very often not the sole source of the problem. Weak quadriceps mean the tendon has to work harder to generate the same amount of force. Tight hamstrings and calves change how load transfers through the knee.
And restricted ankle mobility — a joint two segments away from where you actually feel the pain — can throw off how force travels up the leg on every single landing.
One of the more common moments in our center is what we think of as the compensation conversation. A patient comes in pointing to their knee, convinced that’s where the problem lives. Then we show them something that changes how they think about their body entirely — that their knee pain traces back to ankle mobility restrictions altering how force moves up the leg with every step, or a movement pattern where the knee is absorbing work that the hip should be sharing.
The look on their face when this lands is one of the more satisfying parts of this job. Once someone understands that the site of pain isn’t always the source of pain, they stop chasing the symptom and start addressing what’s actually driving it.
This is exactly why a proper assessment looks beyond the kneecap. We check hip strength, ankle mobility, landing mechanics, and training load, not just the tendon itself.
Key takeaway
Jumper’s knee is a load problem, and load is influenced by everything from your quad strength to your ankle mobility, not just how many times you jumped this week.
Get Your Physiotherapy Treatment Today
Understand your condition better with our detailed physiotherapy assessment, and return to normal life pain-free by addressing your root cause.
Click the button below to book an appointment now!
Treated over 1,000 patients. 30% off first visit
Does Jumper's Knee Heal? (And Why Rest Alone Isn't the Answer)
Yes, jumper’s knee heals and for most people, it heals well.
But here’s an opinion I’ll state plainly, because it matters: rest is the most overprescribed piece of advice in musculoskeletal healthcare.
It feels responsible. It sounds safe. And for the first 24 to 72 hours after a genuine flare-up, it has its place.
But as a long-term strategy, resting an injury and hoping it resolves on its own is roughly as effective as ignoring a warning light on your dashboard. The light is still on. The tendon still hasn’t been trained to handle the load that caused the problem in the first place.
What the Current Evidence Actually Says About Rest and Loading
Tendons don’t get stronger by doing nothing. They get stronger by being loaded progressively, and in the right way.
A systematic review of exercise-based treatments for this exact condition found that isometric exercise (holding a muscle contraction without moving the joint) is effective for short-term pain relief, while heavier progressive strengthening produces better results for long-term pain reduction and function (Lim & Wong, Physiotherapy Research International, 2018). Complete avoidance of load wasn’t the winning strategy in a single one of the studies reviewed.
This lines up with something we see constantly in our center: patients who are told to just rest tend to feel a bit better, stop the aggravating activity, and then flare up again the moment they return to sport because the tendon was never actually trained to tolerate that load.
The pain went away. The underlying weakness didn’t.
How Is Jumper's Knee Treated?
The most effective approach we’ve found — and the one backed by the evidence above — combines two things that are sometimes wrongly presented as competing options: manual therapy and strengthening.
Calming Things Down: The Manual Therapy and Load Management Phase
In the early stage, the priority is reducing pain enough that you can actually do the strengthening work that follows. This might include:
- Manual therapy — techniques like soft tissue release, dry needling, or dry cupping to reduce tension in the surrounding muscles and improve the local tissue environment
- Relative load reduction — scaling back the specific activities provoking pain (not necessarily stopping movement altogether)
- Addressing contributing factors — tight quads, hamstrings, or calves that are adding unnecessary strain to the tendon
Manual therapy genuinely helps here. It reduces pain and creates better conditions for the tendon to start tolerating load again. But it has a ceiling. It cannot build the strength the tendon needs to stop this happening again. That’s a separate job, and it’s the one most treatment plans stop short of finishing.
Rebuilding Capacity: The Strengthening Phase
This is where the actual, lasting fix happens. A tendon that’s been calmed down still needs to be built back up to handle jumping, landing, and sport-specific demand. That means a structured, progressive strengthening program.
One of the clearest examples of this we’ve seen wasn’t even a knee case, but the pattern applies directly.
A patient came to us with hip pain that had been slowing her down as a runner for years. The cause was one we see often in dedicated athletes: a long history of training volume with almost no strength work behind it.
We didn’t just treat the painful area, but we built the surrounding structure that the joint depended on, combining manual therapy for the immediate pain with a progressive strengthening program underneath it.
Her pain reduced, her performance came back, and she now trains completely differently, because she understands that getting stronger and staying pain-free aren’t separate goals. They’re the same goal.
Get Your Physiotherapy Treatment Today
Understand your condition better with our detailed physiotherapy assessment, and return to normal life pain-free by addressing your root cause.
Click the button below to book an appointment now!
Treated over 1,000 patients. 30% off first visit
Jumper's Knee Exercises
Tendons need the right dose of load at the right stage. Not none, and not too much too soon. This is a general framework; if your pain is significant or has been present for a while, it’s worth having a physiotherapist confirm which stage you should actually start at.
Stage 1: Isometric Holds
Best used when pain is more noticeable, to build tolerance without aggravating the tendon further.
Wall sit
Sit against a wall with knees bent to roughly 60–90 degrees, thighs engaged, holding the position. Start with 5 holds of 30–45 seconds, resting between each.
Isometric knee extension
Sit in a chair with your leg out straight, pushing your heel down into a firm surface or against resistance without moving the joint. Hold for 30–45 seconds, repeat 5 times.
Stage 2: Progressive Strengthening
Once isometric holds are comfortable, move into building genuine strength through a fuller range of motion.
Eccentric squat
Standing on a flat surface, slowly lower into a squat over 3–4 seconds, then rise back up. 3 sets of 10–15 reps
Step-downs
Stand on a low step, slowly lower your other foot toward the floor without letting it touch, keeping your knee tracking over your middle toe. 3 sets of 10 per leg.
Bulgarian split squat
With your back foot elevated behind you, lower into a lunge and drive back up. 3 sets of 8–12 per leg. This also builds the hip and glute strength that supports the whole kinetic chain, not just the tendon itself.
Progress the load (added weight, deeper range, more reps) gradually over several weeks, guided by how the tendon responds in the 24 hours after training.
Stage 3: Return to Jumping and Sport
This stage reintroduces the actual demand your sport places on the tendon.
Double-leg hops
Small, controlled hops in place, focusing on soft landings. Start with 2–3 sets of 10.
Single-leg landing
Step off a low box and land on one leg with control, absorbing through the hip and knee together. 2–3 sets of 6–8 per leg.
Sport-specific reintroduction
Gradually return to your actual training like jumping, sprinting, and cutting. Building volume back up over several weeks rather than jumping straight back into full sessions.
How Long Does Jumper's Knee Take to Heal?
There’s no single answer, because it depends on how long the tendon has been struggling and how consistently the strengthening work gets done. As a general guide:
- Mild, early cases: Often settling within a few weeks of consistent isometric and progressive loading work
- Moderate, established cases: Typically 6–12 weeks to feel confident again in daily activity and light training
- More significant or long-standing cases: Often 2–3 months of structured rehab before returning fully to jumping sports, sometimes longer
What consistently predicts a faster, more complete recovery isn’t the specific timeline, but it’s whether someone actually follows through on the strengthening work rather than stopping once the pain has quietened down.
Pain disappearing is not the same as the tendon actually being strong enough to handle what you’re asking of it. That gap is exactly where jumper’s knee tends to come back.
Get Your Physiotherapy Treatment Today
Understand your condition better with our detailed physiotherapy assessment, and return to normal life pain-free by addressing your root cause.
Click the button below to book an appointment now!
Treated over 1,000 patients. 30% off first visit
When to See a Physiotherapist for Jumper's Knee

Get assessed if your pain has lasted more than two to three weeks despite easing off aggravating activity, if:
- it’s affecting your ability to train or work,
- you’re not sure whether you’re dealing with jumper’s knee, runner’s knee, or something else entirely.
A proper physio assessment looks at the tendon itself, but also your hip strength, ankle mobility, landing mechanics, and training history.
In our experience at ONI Physio Fitness, most patients on a combined manual therapy and strengthening program begin noticing meaningful pain reduction within the first 5–6 sessions, with full rehabilitation typically taking somewhere between 12–20 sessions depending on how established the problem is.
Most patients who complete their full program with us return to their sport or activity without ongoing pain.
Get Your Physiotherapy Treatment Today
Understand your condition better with our detailed physiotherapy assessment, and return to normal life pain-free by addressing your root cause.
Click the button below to book an appointment now!
Treated over 1,000 patients. 30% off first visit
Frequently Asked Questions
How do you know if you have jumper's knee?
The clearest sign is localized pain right at the bottom of your kneecap that worsens with jumping, squatting, or stairs, and often eases once you’ve warmed up before returning after activity. A physiotherapist can confirm this with a physical exam.
Does jumper's knee heal on its own?
Mild cases can improve with reduced load, but “on its own” usually means the pain settles temporarily while the underlying weakness in the tendon stays exactly where it was. Without strengthening, it tends to resurface the next time load increases.
What is the fastest way to fix jumper's knee?
There’s no genuine shortcut, but the fastest realistic path is combining short-term load management with an early, progressive strengthening program rather than waiting until pain is completely gone before starting to load the tendon.
Is walking bad for jumper's knee?
No. Walking is generally fine and shouldn’t be avoided. The goal is reducing high-impact, high-load activities like jumping and running, not all movement.
Can you still exercise with jumper's knee?
Yes, and you generally should. Lower-impact strength work and controlled loading exercises are the actual treatment, not something to avoid until you’re pain-free.
Should you stretch for jumper's knee?
Gentle stretching of the quads and hamstrings can help with tightness contributing to the problem, but stretching alone doesn’t build the tendon’s load capacity. It needs to be paired with progressive strengthening.
Can jumper's knee come back after it heals?
Yes, particularly if the strengthening phase was cut short once pain disappeared. The tendon needs to be built back up to the demands of your sport, not just brought back to pain-free.
Do you need surgery for jumper's knee?
Rarely. The large majority of cases respond well to a structured, progressive loading program. Surgery is generally reserved for cases that haven’t responded to a genuine, consistent rehab effort over several months.
Conclusion
If you’re dealing with knee pain that keeps circling back no matter how much you rest it, that’s usually a sign the tendon was calmed down but never actually strengthened.
Start with the isometric holds in Stage 1 this week. No equipment needed beyond a wall and a chair.
If things haven’t meaningfully improved within 2–3 weeks of consistent effort, that’s worth getting properly assessed.
At ONI Physio Fitness in Mont Kiara, we find out what’s actually driving your knee pain, and build the strength to make sure it stays gone.